Twin-Twin Transfusion Syndrom (TTTS) is a rare, life-threatening clinical syndrome that only occurs in identical twins or higher order multiple gestations that share a placenta. TTTS is characterized by one twin developing excessive amniotic fluid volume (polyhydramnios) and the co-twin too little amniotic fluid (oligohydramnios). (The twin with too little amniotic fluid is referred to as the donor twin.)
While the exact cause of TTTS is not known, it is associated with vascular connections on the surface of the placenta and a release of vasoactive mediators by the placenta, which have differential effects on the twins.
For Medical Professionals
Twin-twin transfusion syndrome (TTTS) is a complication of monochorionic multiple gestations in which the circulation of one twin communicates with the circulation of the other twin. Acute clinically relevant TTTS is rare and usually occurs during delivery. It is associated with an acute hemodynamic incident, such as cord compression or rupture of a vessel as in vasa previa (1,2). In these instances, the twins are usually of similar birth weight, but due to acute shift of blood through large chorionic plate vascular anastomoses, usually veno-venous, one twin is pale and the other twin is plethoric.
The lack of agreement on specific diagnostic criteria to define mid-gestation TTTS and the influence of older neonatal criteria have hampered understanding of its pathophysiology and slowed the development of more effective treatment strategies. The donor twin is characterized by oliguria, oligohydramnios or anhydramnios, growth restriction and abnormal umbilical artery Doppler velocimetry. The recipient, on the other hand, is characterized by polyuria, polyhydramnios, abnormal venous Dopplers, cardiac enlargement/failure, and eventually hydrops.
Clinicians caring for women with monochorionic pregnancies should have a strong clinical suspicion for TTTS. Sonographic signs of monochorionic diamniotic twins include a single placenta, a thin dividing membrane, a “T”-sign, and gender concordance. Before ruling out monochorionic diamniotic twins in the case when no dividing membrane is seen, a diligent search for a thin membrane tightly wrapped around one twin should be performed. The following findings are suggestive of the diagnosis of TTTS (meeting all sonographic criteria is not necessary for a diagnosis):
- Discrepancy in amniotic fluid between the amniotic sacs with polyhydraminos of one twin (largest vertical pocket greater than 8 cm) and oligohydraminos of the other (largest vertical pocket less than 2 cm)

- Discrepancy in size of the umbilical cords
- Presence of cardiac dysfunction in the polyhydramniotic twin
- Characteristically abnormal umbilical artery or ductus venosus Doppler velocimetry
- Less specifically, significant growth discordance (often > 20%). Though criteria for TTTS diagnosed in utero were initially derived from neonatal criteria relying on discordant weights (usually > 20%) and hemoglobin levels (usually difference of > 5 g/dL) between the twins, subsequent literature demonstrates that hemoglobin discordance is often not present in mid-gestation and advanced TTTS may be present before the threshold of 20% weight discordance is reached.
In addition to careful sonographic follow-up, mothers of monochorionic diamniotic twins should be alerted that rapid uterine growth, premature contractions and dyspnea may be symptoms of polyhydraminos. The differential diagnosis of TTTS includes uteroplacental insufficiency, growth disturbances due to abnormal cord insertions, intrauterine infection, preterm premature rupture of membranes of one twin, and discordant chromosomal or structural anomalies of one twin.
Cardiovascular compromise occurs in most recipient twins and is a major cause of death for these fetuses (6). In addition, cardiovascular disease in the recipient twin is a significant indirect contributor to morbidity and mortality in the donor co-twin. Echocardiographic examination of the twins is thus an essential component of the initial workup of twin-twin transfusion syndrome as well as follow-up evaluation for progression of the disease and response to treatment. In addition, the study of short-term and long-term cardiovascular effects of various therapeutic interventions is critical.

Recipient twins can develop progressive cardiomyopathy. Although both ventricular dilation and myocardial hypertrophy may occur, the latter predominates and typically only mild evidence of dilatation is seen (6,477). Usually, the right ventricle (RV) is compromised first and to a more significant degree than the left ventricle (LV) (46). In one study of 28 women with TTTS who received echocardiographic evaluation prior to any intervention, right ventricular and/or left ventricular hypertrophy was detected in 58% of recipient twins, and biventricular hypertrophy was observed in 33% of recipient twins (6). Biventricular diastolic dysfunction was present in two-thirds of recipient twins whereas right ventricular systolic dysfunction was present in 35% (9). Atrioventricular valve involvement is also common with moderate insufficiency reported in 71% of recipient twins with structurally normal hearts (48). Moderate to severe tricuspid and mitral regurgitation is more common in Quintero stage III and IV patients (6). Peak velocity of tricuspid and mitral regurgitant jets suggests the presence of ventricular hypertension in echocardiographic data from 39 recipient twins (48). Estimates of RV systolic pressure based on tricuspid regurgitant jet velocity are commonly elevated to 60 to 80 mm Hg, and pressures in excess of 100 mm Hg can be seen in severe cases.
Fetal echocardiography can also be used to assess the response of the recipient twin to fetoscopic laser surgery providing independent confirmation of successful treatment of the TTTS. Habli et al, have shown that in TTTS successfully treated by fetoscopic laser surgery that there is a >10% improvement in the Tei myocardial performance index on post-operative day 5 which only occurs if there has been a complete arrest of the TTTS (49). We routinely obtain a post-operative fetal echocardiogram to confirm that the TTTS has been arrested before sending the patient back to her referring doctor.
Numerous treatments for TTTS have been proposed including selective feticide, cord coagulation, selective abdominal delivery (section parva), placental bloodletting, maternal digitalis, maternal indocin, serial amnioreduction, microseptostomy of the intertwin membrane, and nonselective or selective fetoscopic laser photocoagulation. For decades in the United States, serial amnioreduction had been the most widely accepted therapy for TTTS, but now selective fetoscopic laser photocoagulation is the standard of care with a much more limited role for amnioreduction and even less so for selective reduction.
The first treatment for TTTS that attempted to treat the anatomic basis for the syndrome was reported by DeLia et al. in 1990 (63), who described fetoscopic laser photocoagulatation of vessels crossing the intertwin membrane. At least in theory, this treatment option should be superior since it not only arrests shunting of blood from the donor to the recipient, but also halts the transfer of potential vasoactive mediators. In a subsequent series of patients, DeLia reported in 1995 a survival of 53% in 26 patients (64). While survival was not significantly better than previous reports with serial amnioreduction, the “neurologic outcome” in 96% of survivors was “normal” as assessed by head ultrasounds. Similarly, that same year Ville et al., reported 53% survival with a fetoscopic laser technique which was better than the 37% survival observed with historical controls at the same center with serial amnioreduction (65). They also observed a lower incidence of abnormalities detected by neonatal head ultrasound compared to historical controls.
The non-selective fetoscopic laser technique photocoagulates all vessels crossing the intertwin membrane. This approach may be problematic, as the intertwin membrane often bears no relationship to the vascular equator of the placenta. This non-selective laser photocoagulation of all vessels crossing the intertwin membrane may sacrifice vessels not responsible for the TTTS, resulting in a higher death rate of the donor twin from acute placental insufficiency (66). A selective approach to fetoscopic laser photocoagulation in TTTS has been described by Quintero et al. (66). Unlike the non-selective coagulation technique initially described by DeLia, the selective technique does not photocoagulate every vessel crossing the intertwin membrane. Only direct, arterial-arterial and veno-venous connections are photocoagulated along with any unpaired artery going to a cotyledon with the corresponding vein (and vice versa) going to the opposite umbilical cord. Vessels on the chorionic plate can be differentiated endoscopically because arteries usually cross over veins and are darker in color due to lower oxygen saturation.

In a non-randomized comparison of patients treated by serial amnioreduction at one center and selective laser photocoagulation at another, the overall survival was not statistically significantly different (61% for laser vs. 51% for serial amnioreduction) (67). However, the survival of at least one twin with laser photocoagulation was 79%, while the survival of at least one twin with serial amnioreduction was only 60% (P < 0.05) (67).
The Eurofoetus trial for TTTS conducted by Senat et al. (68) was the first prospective randomized trial that compares the efficacy and safety of treatment of twin-twin transfusion syndrome with laser therapy versus serial amnioreduction. Women presenting between 15 and 26 weeks gestation with polyhydramnios in the recipient twin and oligohydramnios in the donor twin were allowed to participate. Fifty-two percent of patients were stage I or II, 47% were stage III and 1% were stage IV. Enrollment was halted after a planned interim analysis revealed a significantly higher likelihood of survival of at least one twin to 28 days of age (76% versus 56%, P=0.009) and to six months of age (76% versus 51%, p=0.002) in the laser group compared to the amnioreduction group. More infants were alive without neurologic abnormalities detected on neuroimaging studies in the laser group as well (52% versus 31%, P=0.003). The overall survival in the laser arm was 57%. This is consistent with previous reports of non-selective fetoscopic laser (53%) (63,64). This is significantly lower, however, than the survival reported with selective fetoscopic laser (64-68%) (69,70). Of particular concern is the poor survival which was observed in the amnioreduction arm. The overall survival was only 39%, which is significantly lower than previously reported (60-65%) (55,71). Antenatal, peripartum, and neonatal care were provided by the referring hospital and lack of standardization may explain some of these differences (72). The decreased survival in the amnioreduction group may reflect the higher pregnancy termination rate in the amnioreduction group (16 percent versus 0 percent in the laser group). The terminations were requested after the diagnosis of severe fetal complications; it would be instructive to know whether these women were offered cord coagulation as a means of rescuing one baby (72). A reliable assessment of neurologic outcome is critical when assessing the efficacy of treatment for TTTS. While there was a lower rate of abnormality on neurologic imaging in the laser group (7% versus 17%), there was no long-term neurodevelopmental assessment.
Quintero et al. retrospectively examined data from 78 patients treated by serial amnioreduction and 95 patients treated with selective laser photocoagulation with no significant difference in the distribution of patients by stage (69). Perinatal survival was not significantly different in the laser versus amnioreduction group (64.2% versus 57.7%). However, there was an inverse relationship between fetal survival and stage in the amniocentesis group but not in the laser group. For stage IV disease, there was significantly lower fetal survival in the amnioreduction group compared with the laser group (20.6% versus 63.6%, P=0.001). This information has important implications for the evaluation of treatment options and the development of stage-based treatment protocols.
Crombleholme et al, reported the result of the NIH-sponsored TTTS trial which differed significantly from the Eurofoetus trial reported by Senat in that the subjects prior to randomization had to have failed to respond to a single amnioreduction to exclude cases of the single amnioreduction paradox of an incidental septostomy (73). This study was stopped after 40 patients were randomized to fetoscopic laser versus serial amnioreduction when an increase in recipient mortality was noted in the fetoscopic laser arm. This was balanced by similar neonatal mortality in the amnioreduction arm. The two most important findings of this study were that the delay in definitive treatment can allow TTTS cardiomyopathy to progress and secondly, that there is a three-fold increase in recipient mortality with every point deduction in the Huhta Cardiovascular Profile Score used to define the severity of cardiac compromise (73).
Several European centers had observed a high incidence of post-operative twin anemia polycythemia sequence (TAPS) and persistent TTTS. Studies by Lapriore et al suggested that there were a number of communicating placental vessels evident on placental injection studies that had been missed at the time of the fetoscopic laser procedure (74). This led Oepkes and colleagues to suggest the Solomon technique as an adjunct to standard fetoscopic laser procedure in which after the communicating vessels had been identified and treated the intervening area of the placenta was photocoagulated to connect the areas of treatment and prevent small vascular connections from being missed (75). Slaghekke et al, reported the results of a prospective randomized study comparing the use of the Solomon technique to the standard selective fetoscopic laser technique (76). They found that in 274 women randomized the Solomon technique resulted in a significant reduction in post-operative TAPS from 16% to 3% and persistent TTTS from 7% to 1%. This approach has been adopted by many centers in Europe and the United States.
In our experience, the incidence of postoperative TAPS and persistent TTTS is << 1% with our current techniques. There are differences in the approach between the European centers and ours, which may account for this discrepancy. First, we use a fetoscope with a slightly larger lens, which may improve visualization of vessels, particularly small vessels, on the chorionic plate. In addition, we follow a mapping protocol that requires both operators to agree on the nature, size and location of all vascular connections. These are labeled and recorded intra-operatively during the first mapping. During the second mapping, each of the vascular connections is called out in sequence to be identified before being photocoagulated. Then a third mapping is performed to ensure that no vessel has been missed and there has been no recanalization which can occur particularly in large vessels. Since the incidence of complications due to the persistence of vascular connections (TAPS and TTTS) is already << 1%, we have not added the potential risk of laser photocoagulation to the placental area between vascular anastomoses to avoid increasing the risk of preterm premature rupture of membranes.
Dr. Crombleholme has been a pioneer in the treatment of TTTS using selective fetoscopic laser photocoagulation for over 25 years and has performed over 1400 fetal surgical procedures making him one of the most experienced fetal surgeons in the world. His most recent outcomes among 246 patients with fetoscopic laser treatment for isolated TTTS are seen in Figure 1. The outcomes of fetoscopic laser treatment of TTTS are further stratified based on the presence of confounding variables as is the case when TTTS is complicated by selective fetal growth restriction (sFGR), presentation at < 18 weeks, or by a cervical length < 2 cm. Each of these conditions when seen in combination with TTTS, can adversely affect the outcomes as seen in Figure 2.
Figure 1. Dr. Crombleholme’s Outcomes of Selective Fetoscopic Laser Photocoagulation*
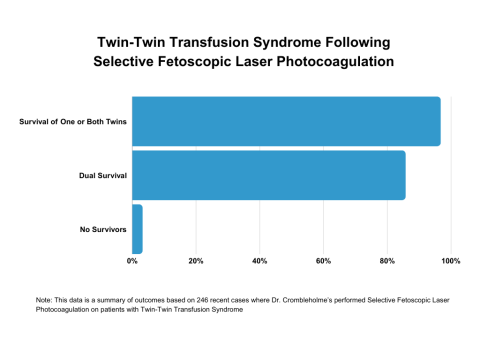
*This data is a summary of outcomes based on Dr. Crombleholme’s 246 most recent cases of performing Selective Fetoscopic Laser Photocoagulation on patients with Twin-Twin Transfusion Syndrome
Figure 2. Dr. Crombleholme’s Outcomes of Selective Fetoscopic Laser Photocoagulation With Confounding Variables*
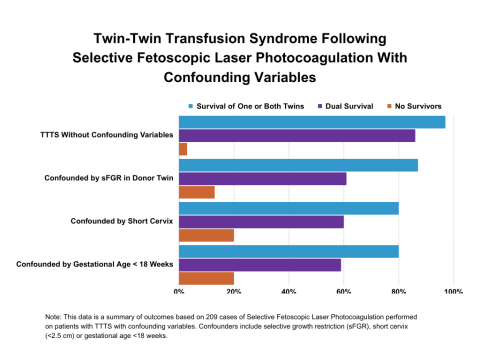
*This data is a summary of outcomes based on 209 cases of Selective Fetoscopic Laser Photocoagulation performed on patients with TTTS with confounding variables. Confounders include selective growth restriction (sFGR), short cervix (<2.5 cm) or gestational age <18 weeks.
These results highlight the impact of sIUGR on survival, particularly of the donor twin. An additional factor, which may influence the donor twin survival in the setting of TTTS complicated by sFGR, is how quickly the laser procedure is performed from photocoagulation of the first vessel to the last. During this period the perfusion of the placenta is altered and there can be an acute transfusion from the donor to the recipient twin. The longer this interval is, the larger the transfusion is likely to be. It is not uncommon post-operatively to see a marked elevation of the donor MCA peak systolic flow velocity on Doppler indicative of anemia in the donor twin if the procedure takes too long. We studied the effect of laser time on fetal survival dividing cases into groups for which laser time was < 5 minutes, between 5 and 10 minutes, and >10 minutes. There was a striking impact on overall survival. There was no effect on recipient survival, which was 92% in all groups. However, donor survival was inversely related to the duration of the laser procedure. In cases in which laser time was > 10 minutes, donor survival was 78%. In the group between 5 and 10 minutes, the donor survival was 85%. In the group < 5 minutes, the survival was 92%. We speculate that in the setting of TTTS complicated by sFGR and small donor placental share, the donor twin can tolerate a small placental share, but not a small placental share complicated by acute anemia. As a result of these data, we now specifically attempt to complete the laser photocoagulation of all communicating vessels in less than five minutes, and out average time is now less than 3 minutes.